Grant M. Tinsley, Patrix S. Harty, Matthew T. Stratton, Madelin R. Siedler and Christian Rodriguez
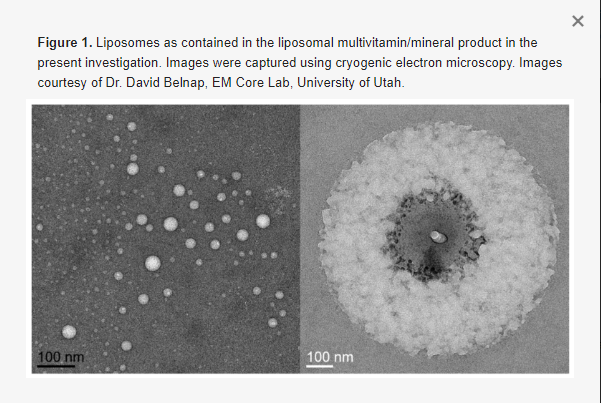
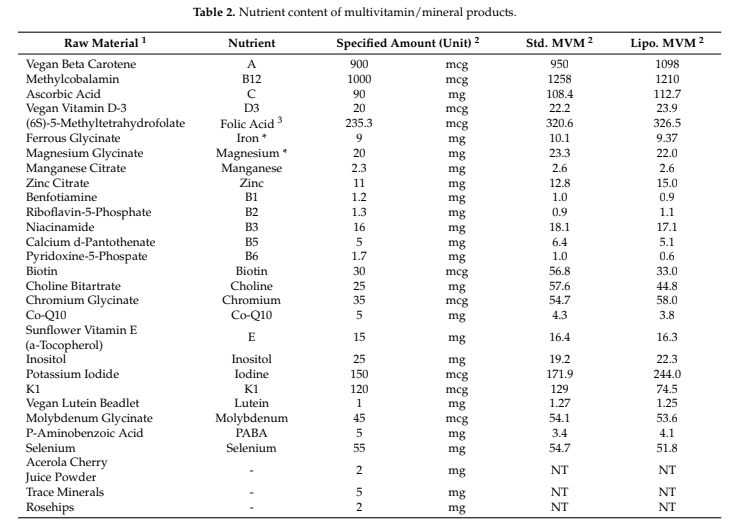
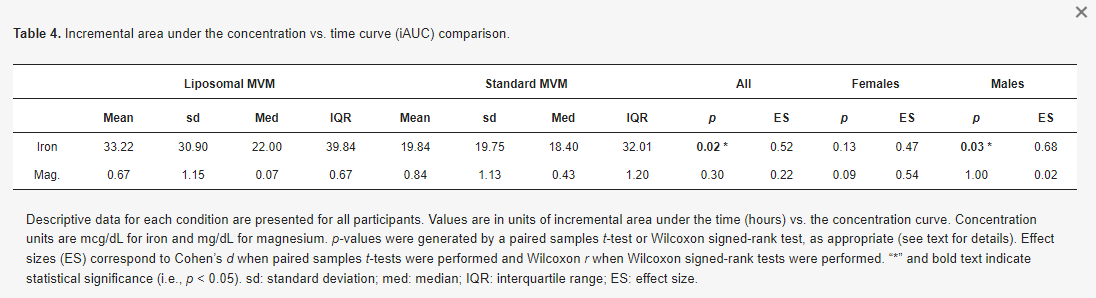
Multivitamin/mineral (MVM) supplements are one of the most popular dietary supplement categories. The purpose of this analysis was to determine if a novel liposomal delivery mechanism improves mineral absorption from an MVM product. In a randomized crossover trial, 25 healthy participants (12 females, 13 males) completed two testing sessions in which blood samples were collected at baseline and 2, 4, and 6 h following the ingestion of either a liposomal MVM or a nutrient-matched standard MVM. Analysis of MVM products indicated an elemental iron content of 9.4 and 10.1 mg (~50% U.S. FDA Daily Value) and an elemental magnesium content of 22.0 and 23.3 mg (~5% U.S. FDA Daily Value) in the liposomal and standard MVM products, respectively. Blood samples were analyzed for concentrations of iron and magnesium using colorimetric assays. Changes in mineral concentrations were analyzed using linear mixed models, and pharmacokinetic parameters were compared between conditions. For iron, statistically significant condition × time interactions were observed for percent change from baseline (p = 0.002), rank of percent change from baseline (p = 0.01), and raw concentrations (p = 0.02). Follow-up testing indicated that the liposomal condition exhibited larger changes from baseline than the standard MVM condition at 4 (p = 0.0001; +14.3 ± 18.5% vs. −6.0 ± 13.1%) and 6 h (p = 0.0002; +1.0 ± 20.9% vs. −21.0 ± 15.3%) following MVM ingestion. These changes were further supported by a 50% greater mean incremental area under the curve in the liposomal condition (33.2 ± 30.9 vs. 19.8 ± 19.8 mcg/dL × 6 h; p = 0.02, Cohen’s d effect size = 0.52). In contrast, no differential effects for magnesium absorption were observed. In conclusion, iron absorption from an MVM product is enhanced by a liposomal delivery mechanism.
This study was a randomized crossover trial examining the pharmacokinetic profiles of mineral absorption from traditional and liposomal MVM formulations in healthy adults. Each participant completed two research visits, which were identical except for which MVM product was consumed. At each visit, participants reported to the laboratory after an overnight fast. After a baseline blood sample was collected, an MVM product was consumed alongside a standardized breakfast. At 2, 4, and 6 h post-ingestion, additional blood samples were collected. Concentrations of iron and magnesium were quantified, and the pharmacokinetic profiles of each nutrient were examined. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Texas Tech University (protocol code 2021-527; date of approval: 22 July 2021). The study was registered on clinicaltrials.gov (identifier: NCT05060367; first posted: 29 September 2021). While the study was originally designed to additionally examine vitamin concentrations, analytical complications at the partner laboratory prevented use of these data.
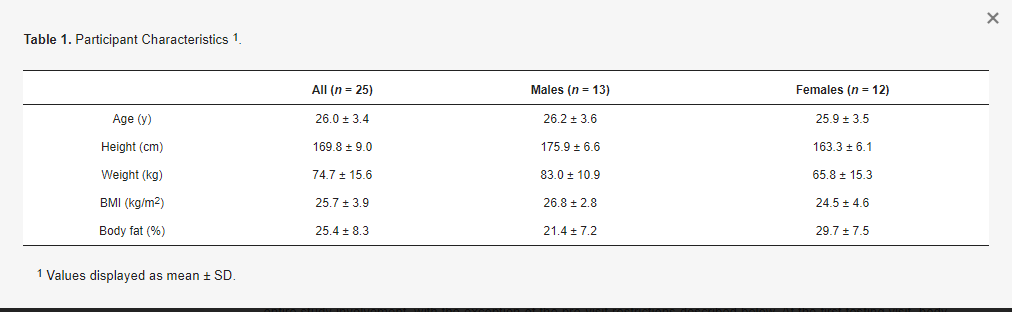
Healthy adult participants were recruited for participation. Inclusion criteria were age of 18 to 65 years, body mass of ≥50 kg (due to blood draws), and anticipated ability to comply with study procedures and scheduling requirements. Exclusion criteria were presence of a disease or medical condition—such as cardiovascular disease, cancer, respiratory disease, gastrointestinal disease, or metabolic disease—or current use of medication that could reasonably influence study outcomes or make participation inadvisable; inability to abstain from medication, supplement, or substance ingestion during the overnight fast and duration of the visit; anticipated inability to provide blood samples; current pregnancy or breastfeeding; and allergy that would prevent safe consumption of the standardized breakfast or MVM products. Written informed consent was obtained from all subjects involved in the study. Participants were asked to follow their normal lifestyle practices—including their typical diet—throughout the entire study involvement, with the exception of the pre-visit restrictions described below. At the first testing visit, body composition was estimated using multi-frequency bioelectrical impedance analysis (Seca mBCA 515/514, Seca, Hamburg, Germany). Participant characteristics.
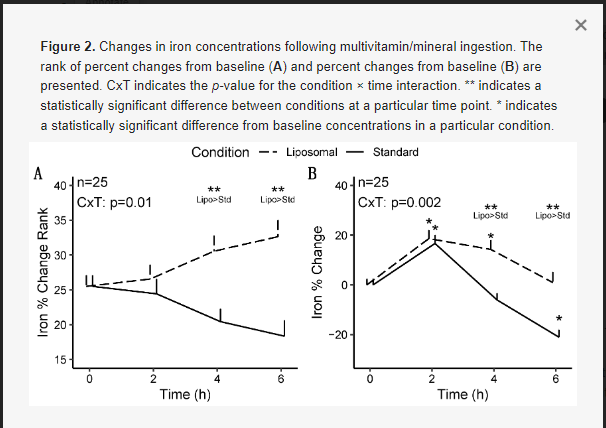
For iron, statistically significant condition × time interactions were observed for rank of percent change from baseline (p = 0.01; Figure 2A), percent change from baseline (p = 0.002; Figure 2B), and raw concentrations (p = 0.02; Appendix A).
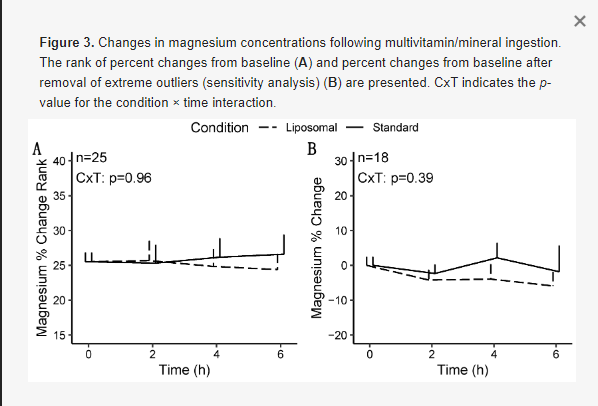
For magnesium, no statistically significant effects of condition, time, or sex were observed in any model (Figure 3), except for a condition × sex × time interaction (p = 0.04) for magnesium changes from baseline in the sensitivity analysis (i.e., following removal of extreme outliers; Table 3). However, follow-up testing revealed no significant two-way interactions or pairwise comparisons after correction for multiple comparisons. Based on the difference in statistical significance of the condition × time × sex interaction, the results of the sensitivity analysis are presented.
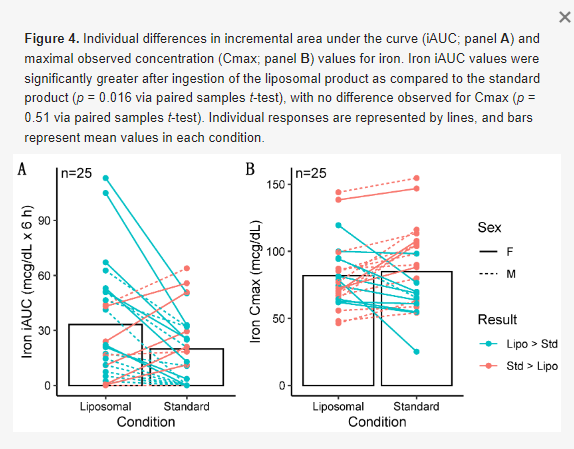
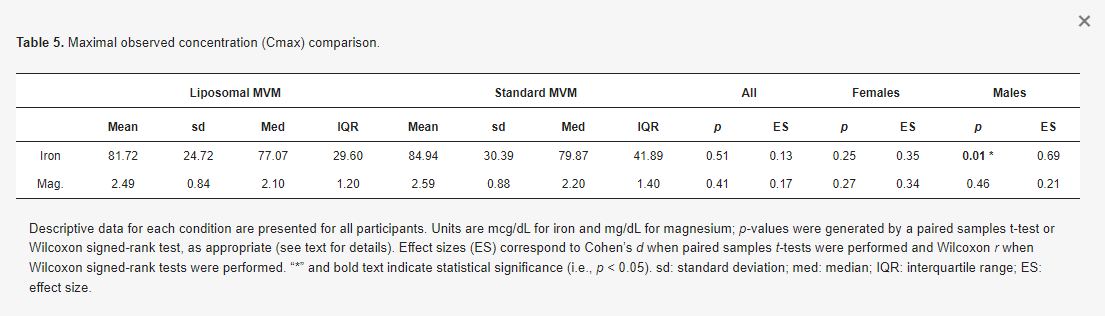
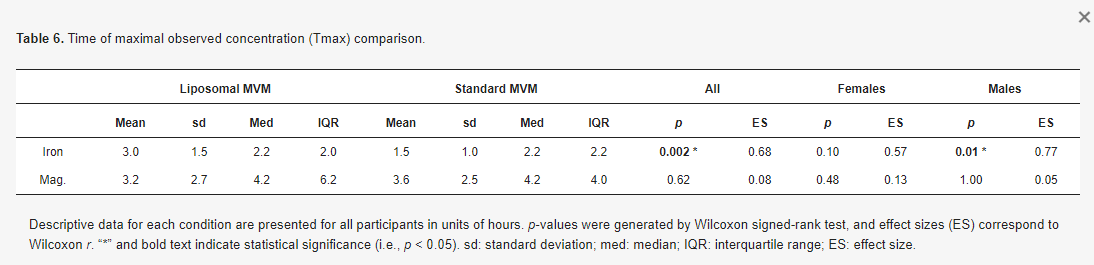
No differences in magnesium iAUC values were observed in the entire sample (p = 0.30, r = 0.22; Table 4; Figure 5), males only (p = 1.0, r = 0.02), or females only (p = 0.09, d = 0.54). Additionally, no differences between conditions for Cmax values were observed in the entire sample (p = 0.41, d = 0.17; Table 5), males only (p = 0.46, r = 0.21), or females only (p = 0.27, d = 0.34). No differences in Tmax were observed for magnesium in the entire sample (p = 0.62, r = 0.08; Table 6), males only (p = 1.0, r = 0.05), or females only (p = 0.48, r = 0.13).

The present randomized crossover trial investigated mineral absorption from liposomal and non-liposomal MVM products. As hypothesized, improved iron absorption was observed following ingestion of the liposomal product. Specifically, larger changes in iron from baseline—using both percent changes and ranks of percent changes—were observed in the liposomal condition at 4 and 6 h after MVM ingestion. Additionally, the iAUC for iron was 50% greater following ingestion of the liposomal MVM product. No differences between conditions were observed for magnesium absorption. Importantly, the dose of iron contained in the MVM product represented a relevant dose, whereas the relative dose of magnesium was much lower. The quantity of elemental iron in the MVM products represented ~50% of the 18-mg Daily Value used by the U.S. Food and Drug Administration (FDA) for nutrition labeling purposes [18]. Additionally, the doses of elemental iron used in the present study (9.4 to 10.1 mg) meet the Recommended Dietary Allowance (RDA) for males of all ages, except 14–18 years (RDA: 11 mg/d), and meet or make a substantive contribution to the recommended intake for adult females (RDA: 8 to 18 mg/d, depending on age, in non-pregnant females; 27 mg/d in pregnant females). This indicates that the quantity of iron contained in the MVM product is meaningful relative to daily intake recommendations and supports the relevance of the improved absorption seen with the liposomal formulation. In contrast, the doses of elemental magnesium in the present study were low relative to daily intakes (22 to 23.3 mg vs. U.S. FDA Daily Value of 420 mg; ~5% of Daily Value) [19]. This may indicate that the influence of liposomal delivery on magnesium absorption should be further investigated with higher doses, perhaps through a standalone magnesium supplement due to practical limitations on absolute quantities of ingredients in MVM products. Preliminary research with a form of liposomal magnesium supports this contention, as one study indicated enhanced absorption as compared to non-liposomal forms following ingestion of 350 mg magnesium (i.e., ~15-fold higher than the dose in the present investigation) [35]. This research was conducted within the context of single-nutrient products, in contrast to the present investigation, which examined nutrient absorption from MVM products.
The observed improvement in iron absorption with liposomal packaging is notable for several reasons. First, iron is essential for a host of physiological functions, ranging from oxygen handling as part of hemoglobin and myoglobin, to hormone synthesis and support of normal cellular function [18]. Second, while previous research has indicated benefits of liposomal delivery for absorption of vitamins [14,15,16,17], there is little information regarding mineral absorption. As such, the present investigation demonstrates the promise of liposomal technology in this regard. Third, the benefit to iron absorption was observed in the context of a relatively bioavailable source of iron, ferrous glycinate. Previous research has demonstrated superior bioavailability of ferrous glycinate as compared to iron salts, such as ferrous sulfate [36,37,38]. As such, it is notable that liposomal packaging further improved absorption. While speculative, it is possible that the enhancement of absorption with liposomal packaging would be even more evident with less bioavailable forms of nutrients. Fourth, the global impact of inadequate iron intake and international recommendations for iron supplementation indicate the importance of using the most effective supplement form. The WHO estimated that one in three non-pregnant women, corresponding to ~500 million individuals, were anemic in 2011, and that iron deficiency likely contributed to at least half of these cases [20]. Correspondingly, a 2016 WHO report recommends daily iron supplementation in menstruating adult women and adolescent girls living in settings where anemia is prevalent [20]. It is well established that groups at risk for inadequate iron intake include adolescent, pregnant, and premenopausal women, as well as infants and children [18]. Racial disparities have also been reported, with higher rates of depleted iron stores in Mexican American and non-Hispanic Black pregnant women [39]. Additionally, those in food-insecure homes are more likely to experience inadequate iron intake [40]. Collectively, these and other lines of evidence indicate the importance of iron supplementation in several contexts and demonstrate the need for effective supplementation formulations.
While few investigations have examined the acute absorption properties of minerals encapsulated in liposomes, some have indicated promise for these products for health improvements following chronic supplementation in clinical conditions [41,42,43,44]. A randomized trial in chronic kidney disease patients demonstrated similar increases in hemoglobin after 3 months of treatment with oral liposomal iron supplements or intravenous iron administration, along with a lower incidence of adverse effects with oral supplementation [41]. A separate single-arm trial in patients with chronic kidney disease indicated that a liposomal iron preparation was well tolerated and increased hemoglobin, relative to baseline, after 12 months of supplementation [42]. In a single-arm trial conducted in anemic patients with inflammatory bowel disease, 62% of patients completing treatment with oral liposomal iron supplements increased hemoglobin above a prespecified threshold or presented with hemoglobin normalization after 8 weeks of treatment; improvements in quality of life and reductions in fatigue were also noted [43]. Finally, a randomized trial in pregnant, non-anemic women indicated that liposomal iron was effective for elevating hemoglobin and ferritin concentrations as compared with control [44]. While these investigations demonstrate the potential utility of liposomal iron formulations, several trials are limited by a lack of control or comparison groups. As such, additional research is needed to investigate the potential for unique health effects in various clinical populations, as well as in the general population.
While both multi-nutrient (e.g., MVM) and single-nutrient supplements may exhibit benefits in specific contexts, the investigation of individual nutrient absorption from an MVM product is relevant due to the notable prevalence of MVM supplementation. As previously noted, NHANES data indicate that MVM products are consumed more frequently than any other type of dietary supplement [3]. Importantly, the bioavailability of individual nutrients from an MVM product may be dissimilar to absorption from single-nutrient products due to the specific matrix of nutrients and corresponding nutrient–nutrient interactions within an MVM [10]. As such, and due to the dearth of bioavailability data for MVM products, investigations that directly quantity single nutrient absorption from an MVM product—such as the present report—are warranted.
A major strength of the present investigation is the use of COA to objectively verify the nutrient content of the liposomal and standard MVM products. Interestingly, the benefits of liposomal iron delivery are further highlighted by the fact that the elemental iron content was 7.5% (0.73 mg) lower in the liposomal MVM than the standard MVM, based on the COA. Similarly, the elemental magnesium content was 5.7% lower in the liposomal MVM product. Additional strengths of this study include the rigorous procedural standardization during data collection and multifaceted statistical analysis. Limitations of the present work include the inability to examine additional outcomes; the low dose of magnesium, which limits the relevance of this nutrient as a study outcome; the relatively young, healthy, and homogenous sample; and the limited number of time points utilized. Additionally, the monitoring period of 6 h following MVM ingestion could be a limitation, as a statistically significant difference in iron changes between conditions was present at this time point; therefore, the full duration of differential iron changes could have persisted beyond this point. However, interestingly, iron had returned to near baseline levels in the liposomal condition by 6 h after MVM ingestion, whereas iron concentrations fell below baseline levels in the standard MVM condition. An additional consideration is that while the two MVM products were designed with identical specified amounts of each nutrient, minor differences between the standard and liposomal MVM products were observed through the laboratory COA results. While this may be unavoidable for products with many ingredients and small doses of each individual ingredient, it is worth noting. However, as mentioned, the dose of iron (as well as magnesium) was actually lower in the liposomal MVM, indicating the positive results observed were not due to this slightly different dose. Lastly, the potential influence of compounds within the MVM products on iron and magnesium absorption should be considered. Based on the potential for complex, and largely unknown, interactions between compounds within MVM products [10], the results of the present study could have differed if compounds were studied in isolation.
In conclusion, the present randomized crossover trial demonstrated improved iron absorption following ingestion of iron from a novel liposomal MVM as compared to a standard MVM. This finding helps to determine optimal iron supplementation strategies and demonstrates the potential for liposomal packaging to benefit mineral absorption. Future research should continue to examine the potential utility of liposomal delivery of micronutrients in a variety of populations, for both MVM formulations and single-nutrient products.



